NOTE: Our laboratory offers multiple testing options for non-small cell lung cancer. Please see our Lung Cancer overview page.
OVERVIEW
Anaplastic lymphoma kinase (ALK) is a receptor tyrosine kinase in the insulin receptor family. Rearrangements in the ALK gene are found in approximately 3-5% of non-small cell lung carcinomas (NSCLC) of non-squamous, non-neuroendocrine histology, and almost exclusively in those that do no harbour an EGFR or KRAS mutation or ROS1 fusion.
The most common ALK rearrangement involves a paracentric inversion of the short arm of chromosome 2 that results in the fusion of 5’ EML4 with 3’ ALK. The resulting fusion generates a constitutively active tyrosine kinase. Alternate fusion partners with ALK have also been identified and unbalanced rearrangements are common. Constitutively active ALK fusions are oncogenic and NSCLC carrying these rearrangements are sensitive to ALK tyrosine kinase inhibitor therapies.

INDICATION
- Stage IIIB/IV non-small cell, non-neuroendocrine lung adenocarcinoma with equivocal ALK IHC.
TEST REQUIREMENTS
ALK FISH is typically performed as a confirmatory test for equivocal (2+) ALK IHC results. Confirmatory FISH testing is not required for positive or negative ALK IHC results.
- Completed CGL Solid Tumour Testing requisition form:
- ALK screening by IHC is automatically performed in combination with Focus Panel testing
- FFPE Tumour specimen (see Specimen Guidelines, Cytogenetics test type)
- A minimum of 10% tumour content and at least 200 nuclei is required
TURN-AROUND TIME
Results are reported within fourteen days from receipt of specimen and completed requisition form.
RESULTS REPORTING
- Specimens are reported as Positive for a rearrangement, Negative for a rearrangement, or Negative for a rearrangement – extra signals.
- Specimens with inadequate tumour tissue may be cancelled by the reviewing pathologist prior to receipt in CGL.
METHOD
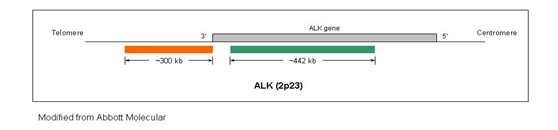
FISH analysis is performed on the provided paraffin embedded tissue using the ALK (2p23) dual-colour, break-apart probe (Vysis).
REFERENCES
- Melosky et al. Current Oncology (2018) PMID:29507487